




- 19
- 5
I remember watching a youtube video about how eating very little is bad for you, but doing a complete fast is good because biology or smth.
Is this true?







- 43
- 59
You look like a garbage goblin always baby 😍 pic.twitter.com/WLZzQq2gP1
— Flinn (@hasnteatentoday) October 20, 2022
both of these are good but im referring to the bottom one





- 59
- 60
](/images/16663604883204331.webp)
Sharon Maxwell spent much of her life trying to make herself small. Her family put her on her first diet when she was 10. Early on Saturday mornings, she and her mother would drive through the empty suburban streets of Hammond, Ind., to attend Weight Watchers meetings. Maxwell did her best at that age to track her meals and log her points, but the scale wasn’t going down fast enough. So she decided to barely eat anything on Fridays and take laxatives that she found in the medicine cabinet.
Food had long been a fraught subject in the Maxwell household. Her parents were also bigger-bodied and dieted frequently. They belonged to a fundamentalist Baptist megachurch where gluttony was seen as a sin. To eat at home was to navigate a labyrinth of rules and restrictions. Maxwell watched one time as her mother lost 74 pounds in six months by consuming little more than carrot juice (her skin temporarily turned orange). Sometimes her father, seized with a new diet idea, abruptly ransacked shelves in the kitchen, sweeping newly forbidden foods into the trash. Maxwell was constantly worried about eating too much. She started to eat alone and in secret. She took to chewing morsels and spitting them out. She hid food behind books, in her pockets, under mattresses and between clothes folded neatly in drawers.
Through Maxwell’s teenage years and early 20s, eating became even more stressful. Her thoughts constantly orbited around food: what she was eating or not eating, the calories she was burning or not burning, the size of her body and, especially, what people thought of it. Her appearance was often a topic of public interest. When she went grocery shopping for her family, other customers commented on the items in her cart. “Honey, are you sure you want to eat that?” one person said. Other shoppers offered unsolicited advice about diets. Strangers congratulated her when her cart was filled with vegetables.
As she grew older, people at the gym clapped and cheered for her while she worked out. “People would say: ‘Go! You can lose the weight!’” she says. While eating in public, other diners offered feedback — and still do to this day — on her choices, a few even asking if she wanted to join their gym. Some would call her names: Pig, Fatty. Sometimes people told her she was brave for wearing shorts, while others said she should cover up. She was always aware, whether she wanted to be or not, of how others viewed her body.
Maxwell tried just about every diet she could find: juice cleanses, Atkins, SlimFast, South Beach, Mediterranean, Whole30 and Ezekiel, a regimen based on biblical references. She tried being vegetarian and vegan and paleo. She tried consuming less than 500 calories a day and taking HCG, a fertility hormone rumored to suppress appetite but flagged by the F.D.A. as risky and unproven for weight loss. During periods of religious fasting at her church, she would take the practice to an extreme, consuming nothing but water for days (and on one occasion, two weeks). “I passed out a few times, but I did it,” she says. Sometimes she exercised more than three hours a day in high-intensity interval-training sessions and kickboxing classes. Eventually, she started vomiting up her food.
Every day, Maxwell stepped on the scale and internalized the number as a reflection of her self-worth. Often, the number on the scale went down. But if she let up on her rigid food rules even briefly, the number shot back up like a coiled spring. “I just cycled through that,” she says, “but it became harder and harder each time to get the weight off.”
During the many years of dieting and deprivation, Maxwell experienced mysterious health problems. For a decade, starting when she was 16, she almost never had her period. She was always cold. She often had dizzy spells and occasionally passed out in class. When she was in college, she fainted three times in one day and was taken to the emergency room. For an appointment with an endocrinologist one year, Maxwell took a purse full of small plastic bags. Each one contained a day’s worth of hair, clumps that accumulated in her brush or had fallen in the shower drain. Her head was pocked with bald spots. The doctor was pleased with her weight loss and, to her memory, didn’t seem too concerned about her other symptoms. “Anything that made the scale go down,” Maxwell says, “I was given a pat on the back.”
Four years ago, at the age of 25, Maxwell walked into her primary-care doctor’s office near Scottsdale, Ariz., where she lived and worked as a middle school teacher. She was there for an annual physical, and she was prepared to be told to lose weight, as she had almost always been instructed. But this time, the doctor, an osteopath, started asking unusual questions. Maxwell’s blood work showed abnormally low iron and electrolyte levels. The doctor asked Maxwell what she was eating and what she was doing in relationship to food. Was she starving herself? Was she vomiting on purpose? Maxwell was surprised by this line of questioning. “These are things I had hidden my whole life from my family, my friends, doctors,” she says.
The osteopath told her she thought Maxwell had an eating disorder and suggested arranging treatment right away. Maxwell would later be diagnosed with atypical anorexia nervosa, an increasingly common yet little known eating disorder that shares all the same symptoms as anorexia nervosa, except for extreme thinness. Just as many people, and possibly many more, suffer from atypical anorexia.
At the physical, Maxwell stared at her doctor in disbelief. She always thought that eating disorders were for skinny people. “I laughed,” she says. “I don’t use language like this any longer, but I told her she was crazy. I told her, ‘No, I have a self-control problem.’”
For centuries, the eating disorder that would become known as anorexia nervosa mystified the medical community, which struggled to understand, or even define, an illness that caused people to deliberately deprive themselves of food. As cases rose over the course of the 19th and 20th centuries, anorexia was considered a purely psychological disorder akin to hysteria. Sir William Withey Gull, an English physician who coined the term “anorexia nervosa” in the late 1800s, called it a perversion of the ego. In 1919, after an autopsy revealed an atrophied pituitary gland, anorexia was thought to be an endocrinological disease. That theory was later debunked, and in the mid-20th century, psychoanalytic explanations arose, pointing to sexual and developmental dysfunction and, later, unhealthy family dynamics. More recently, the medical field has come to believe that anorexia can be the product of a constellation of psychological, social, genetic, neurological and biological factors.
Since anorexia nervosa became the first eating-related disorder listed in the Diagnostic and Statistical Manual of Mental Disorders in 1952, its criteria have shifted as well. Initially, anorexia had no weight criteria and was classified as a psychophysiological disorder. In a 1972 paper, a team led by the prominent psychiatrist John Feighner suggested using a weight loss of at least 25 percent as a standard for research purposes, and in 1980, the D.S.M. introduced that figure in its definition (along with a criterion that patients weigh well below “normal” for their age and height, although normal was not defined). Doctors who relied on that number soon found that patients who had lost at least 25 percent of their body weight were already severely sick, so in 1987, the diagnosis was revised to include those who weighed less than 85 percent of their “normal” body weight (what qualified as normal was left to physicians to decide). In the 2013 D.S.M., the criteria shifted again, characterizing those who suffer from anorexia as having a “significantly low weight,” a description that would also appear in the 2022 edition.
In that 2013 edition, a new diagnosis appeared — atypical anorexia nervosa — after health care providers noticed more patients showing up for treatment with all the symptoms of anorexia nervosa except one: a significantly low weight. Those with atypical anorexia, doctors observed, suffer the same mental and physical symptoms as people with anorexia nervosa, even life-threatening heart issues and electrolyte imbalances. They restrict calories intensively; obsess about food, eating and body image; and view their weight as inextricably linked to their value. They often skip meals, eat in secret, adhere to intricate rules about what foods they allow themselves to consume and create unusual habits like chewing and spitting out food. Others exercise to the point of exhaustion, abuse laxatives or purge their meals. But unlike those diagnosed with anorexia, people with atypical anorexia can lose significant amounts of weight but still have a medium or large body size. Others, because of their body’s metabolism, hardly lose any weight at all. To the outside world, they appear “overweight.”
Starting in the mid-2000s, the number of people seeking treatment for the disorder rose sharply. Whether more people are developing atypical anorexia or seeking treatment — or more doctors are recognizing it — is unknown, but this group now comprises up to half of all patients hospitalized in eating-disorder programs. Studies suggest that the same number of people, even as many as three times as many, will develop atypical anorexia as traditional anorexia in their lifetimes. One high estimate suggests that as much as 4.9 percent of the female population will have the disorder. For boys, the number is lower — one estimate was 1.2 percent. For men, it is likely even lower, though little research exists. For nonbinary people, the number jumps to as high as 7.5 percent.
Across the board, the pandemic exacerbated eating disorders, including typical and atypical anorexia, through increased isolation, heightened anxiety and disrupted routines. Hospitals and outpatient clinics in the United States and abroad reported the number of consultations and admissions doubling and tripling during Covid lockdowns, and many providers are still overbooked. “Almost all of my colleagues, we’re at capacity,” says Shira Rosenbluth, an eating-disorder therapist who specializes in size- and gender-diverse clients. They are seeing clients who practice more extreme food restriction and experience more intense distress around body image and eating habits. “The demand has increased, the level of severity has increased,” Rosenbluth says. “We’ve never seen waiting lists like this for treatment centers.”
](/images/16663606658550692.webp)
Despite its prevalence, atypical anorexia is still considered widely underdiagnosed and under-researched, and many primary-care doctors have never heard of it. “Some people being at a standard body weight or overweight can be perplexing to the untrained eye,” says Karlee McGlone, senior manager of admissions and outreach for U.C. San Diego Health Eating Disorders Center. “It is still a surprise for nonspecialized clinicians.”
Patients, too, are in the dark about atypical anorexia. “Most people in higher-weight bodies are shocked to hear that they have anorexia,” says Rachel Millner, a psychologist based in Pennsylvania who specializes in eating disorders among people with larger bodies. “Nobody ever told them that you can be in a higher-weight body and have anorexia, and they’re convinced that their problem is their weight.”
In 2020, Erin Harrop, an assistant professor of social work at the University of Denver, completed a survey of 39 people with atypical anorexia, most of whom were obese, and found that participants endured the disorder for an average of 11.6 years before seeking help. They lost an average of 64 pounds, and a quarter of the group had yet to receive treatment. (By comparison, the treatment delays for anorexia are, on average, 2.5 years; for bulimia, 4.4 years; and for binge-eating disorder, 5.6 years, according to a 2021 review.)
To make it easier for people with atypical anorexia to be screened, treated and insured, there’s a growing movement in the field to collapse the categories of anorexia and atypical anorexia into one — to no longer see them as separate illnesses, to decouple anorexia from its virtually synonymous association with thinness. “For years, we have thought about anorexia nervosa in one way,” says Carolyn Costin, an eating-disorder therapist who founded an eating-disorder treatment center and is a co-author of “8 Keys to Recovery From an Eating Disorder.” “But the way people think about it and how they want to define it is changing. It would be a paradigm shift within the field.”
Many, however, are fiercely resistant to letting go of the metric of weight. It would require altering the organizing principle by which the public and the greater medical field conceive of the condition. It would also require recognizing that anyone, in any body, can starve themselves into poor health — and you’d never know it by looking at them.
It took Maxwell a long time to process that she had an eating disorder. She had been so steeped in the gospel of dieting that it was hard to accept that restricting her food was not unequivocally healthy. But as her doctor instructed, she began making visits to the hospital for intravenous fluids and started taking iron supplements. At night, she began attending outpatient sessions at Liberation Center, a now-shuttered facility in Phoenix, where she ate dinner with other clients and attended group therapy. The staff at Liberation told her she needed more intensive treatment and recommended attending a residential program.
In the summer of 2018, after teaching through the rest of the school year, Maxwell agreed to go to a center in Monterey, Calif., that was covered by her insurance. A day after she arrived, however, her insurance rescinded approval: Because of her weight, the company didn’t believe she was sick enough to meet the criteria for residential care for eating disorders. She was at once ashamed and incensed. Her aunt drove five hours to pick her up, and she spent much of the next 10 days on the phone with the insurance company.
Her insurance eventually authorized her to go to another facility, the Center for Discovery Rancho Palos Verdes, which sits on the Southern California coast. Maxwell’s three-month stay would consist of group meals, outings to restaurants to practice dining in public settings, yoga and therapy. “I went with the expectation that as soon as I walked in the door, they would be the people who would help me finally become thin once and for all,” she says. Instead, on her first day, a dietitian at the center explained that she would need to eat three balanced meals and three snacks a day to recover. Her treatment plan also required that she abstain from almost all forms of exercise so her system could recalibrate. Maxwell panicked. She had never consistently eaten that much in her entire adult life, and she still felt that her body was a problem to be fixed.
Maxwell already harbored a deep mistrust of the mental-health profession. When she was growing up, she remembers a pastor at her church preaching that psychiatry was the work of the devil. The message seemed to be that anxiety was sinful, a sign of faithlessness. Maxwell had left her church two years earlier, but its lessons were still lodged deeply in her mind. She couldn’t abandon her long-held belief, one that her doctors reinforced for much of her life, that thinness was the primary measure of health.
Maxwell forced herself to go along with each step of the treatment program. She tried to eat three meals and three snacks a day, even though it caused her excruciating fear. For years, her thinking had revolved tightly around food and exercise; and during twice-weekly individual therapy sessions and daily group therapy, she tried to learn how to redirect these thoughts. She started to talk about the self-judgment, shame and childhood trauma that led to rigid behaviors and an overreliance on control, both central features of restrictive eating disorders.
About five or six weeks into treatment, it dawned on her just how much damage she had done to herself. Her esophagus burned from years of purging. She experienced heart palpitations and was often dizzy from orthostatic hypotension (a type of low blood pressure that leads to dizziness and fainting), and her hair and nails were thin and brittle from malnutrition. “I started to realize, holy shit, this is real,” she says. “I started to see what it had done to my body, the magnitude of it.”
Over the ensuing weeks, Maxwell began eating enough food that the staff allowed her to go on walks and swim, not to burn calories but as a part of learning how to live a balanced life. Her physical symptoms started to ease. Her vital signs and blood work improved. She felt less dizzy, her heartbeat more regular. She got her period back for the first time in a decade. And perhaps most surprising, she was not gaining weight despite eating more food.
To help her overcome her self-judgment, a nurse suggested that she look in the mirror and express what she liked about her body. At first, Maxwell couldn’t think of what to say. She could hardly make eye contact with her own reflection. But eventually she thought of something. “I’m grateful for my curly hair,” she said, looking at the nurse in the mirror.
When a human body is starved for long enough, it undergoes a complex series of biological, metabolic and hormonal changes to ensure its own survival. Every system moves to conserve energy, and the body begins to mine muscle and fat for glucose to keep the heart running and the brain functioning. The metabolism slows, which is why some people can eat very little and hardly lose any weight. Digestion simmers down, sometimes causing gastrointestinal trouble, and body temperature plummets while blood flow decreases. Many people who chronically undereat shiver with cold, their hands and feet feeling especially icy. If malnutrition worsens, their hair becomes fragile and falls out and muscle mass dwindles, including within the heart.
People with severe anorexia of any kind can have orthostatic hypotension, heart rates lower than 60 beats per minute and electrolyte imbalances that may cause arrhythmias or even lead to cardiac arrest. Eventually a malnourished body can shut down the production of s*x hormones. From what little research on atypical anorexia exists, the medical complications appear to be the same as anorexia and occur in similar rates across body sizes, with the exceptions of bone density loss and low blood sugar, which are worse in those who are emaciated. Recent research has found that body size is a less relevant indicator of the severity of both eating disorders than other factors, including the percentage of body mass lost, the speed of that loss and the duration of the malnourished state.
Among scientists, there is consensus that atypical anorexia and anorexia share the same medical and nutritional issues, but one of the big remaining questions is whether the psychopathology is the same (some clinicians believe that it is, but minimal research exists to confirm this). In the slim populations they have studied, psychologists have observed a grim momentum to the illness: Sufferers lose just a few pounds and then, all of the sudden, they compulsively want to lose more, as if a mental switch flips. Genetic predispositions may explain why some people lose weight and their minds tip into disordered eating while others do not. Immediate female family members of a patient with anorexia nervosa are 11 times as likely to develop it as females in the general population, according to one study.
Side note: fittingly, the file name given by the NYT for the first picture is 23mag-anorexia-superJumbo.jpg.webp 





- 42
- 77
what's her username here? 
An Australian woman has sparked a wave of internet backlash after posting a photo of herself on an American Airlines flight complaining about having to sit beside two "obese people."
Sydney Watson, an Australia-American conservative political commentator, took to Twitter to share her experience while on a three-hour American airline flight.
Sydney Watson complained to American Airlines about being 'wedged between two obese people.'
"I am currently --- literally --- WEDGED between two OBESE people on my flight," Watson tweeted.
"This is absolutely NOT acceptable or okay. If fat people want to be fat, fine. But it is something else entirely when I'm stuck between you, with your arm rolls on my body, for 3 hours."

https://x.com/SydneyLWatson/status/1579609743244800006
Watson's complaint was met with immediate backlash from other social media users, who accused her of being extremely fatphobic and downright mean.
"This is my worst nightmare as a fat person who is not rich. I would hate to see a picture of my fat body on a stranger's Twitter because I want a vacation," one user wrote in response to Watson's tweet.
However, Watson doubled down on her post, saying that she doesn't care 'if this is mean.'
"I can't even put the arm rests down on either side because there's no f-king room. I'm sick of acting like fatness to this extent is normal. Let me assure you, it is not," she wrote.
The official Twitter account for American Airlines quickly responded to Watson's viral post, rebuffing her claims.
"Our passengers come in all different sizes and shapes. We're sorry you were uncomfortable on your flight," the airline wrote.
Though, a week later, Watson, who demanded "reparations" for being forced to sit in the middle seat, received an email from American Airlines offering her compensation.
In the email shared by Watson, the airline apologized for the discomfort and offered her a $150 coupon.
"We do our best to avoid uncomfortable situations regarding seats. I can understand your disappointment with the situation not being remedied to your satisfaction. It seems that our Flight Attendants were not able to make changes to the seating arrangement," the email stated.
In response to American Airlines offering her the coupon, Watson continued her tirade against the airline company, tweeting that she'd rather give the coupon "to someone who needs PT or a gym membership."


- 38
- 43
Kid core pic.twitter.com/fLqqpUi94E
— Charlotte (@charlottexoxooo) July 12, 2022
watch the “kidcore” one for the fatty idk why the other one showed up

- 8
- 18
crusty ass nails pic.twitter.com/5ZHgrVShu2
— ًً (@irisdisease) July 17, 2022


 irl
irl
- 39
- 108


 the energy needed to raise the temperature of 1 gram of water through 1 °C (now usually defined as 4.1868 joules).
the energy needed to raise the temperature of 1 gram of water through 1 °C (now usually defined as 4.1868 joules). - 14
- 39





 If you have to be a complete beautiful woman you have to be physically fit. Definitely not fat. Fat is ugly, Queen tells it like it is, no one is capable of saying this in CurrentYear+7
If you have to be a complete beautiful woman you have to be physically fit. Definitely not fat. Fat is ugly, Queen tells it like it is, no one is capable of saying this in CurrentYear+7
- 14
- 42
Some pc sneed from my Indian Deuxmoi https://old.reddit.com/r/BollyBlindsNGossip/comments/y6ry54/rekha_if_you_have_to_be_a_complete_beautiful/



.webp?h=8 "Merry Fistmas!")
- 4
- 31
Well, here's the email I got from American Airlines. pic.twitter.com/bfa2jwoZYE
— Dr. Sydney Watson (@SydneyLWatson) October 17, 2022




 Trans Species Okapi
Trans Species Okapi - 70
- 221
That movie was 50% just fat people jokes lol and I loved it.
Ecoterrorism against deathfats when?


 God bless this mess
God bless this mess 



- 36
- 66
Scooters everywhere, wheelchairs all over, and worst of all—grown-butt children who are like 11 years old being pushed around in fortified, oversized strollers.
When did parents start pushing around their able-bodied, older children like this? These future braps and heart disease patients are being carted around while they pig out on candy and zone out on their iPads and I don't understand why parents encourage this behavior. It's over for whatever generation this is 
I hope the government starts treating childhood obesity as a national security threat and starts making these little piglets take care of their health
Less  and
and 
More  and
and 
- BernieSanders : poorcel cope, just buy two seats next time cute twink
- THOMAS : >publictransportcel alert

- 40
- 70
I'm absolutely pissed, I reserved a seat specifically to not have to deal with the unwashed masses. Sadly I am slim and the seat next to me was the only free one, so I am currently fighting not to throw up
He just pulled out a clear bag of cold chicken nuggets, I think he brought them from home?
He smells like a carcass and he's German so I'm certain this is some fetish he's making me participate in
Good vibes requested and appreciated, I am on this train for 2.5 more hours






- 6
- 6
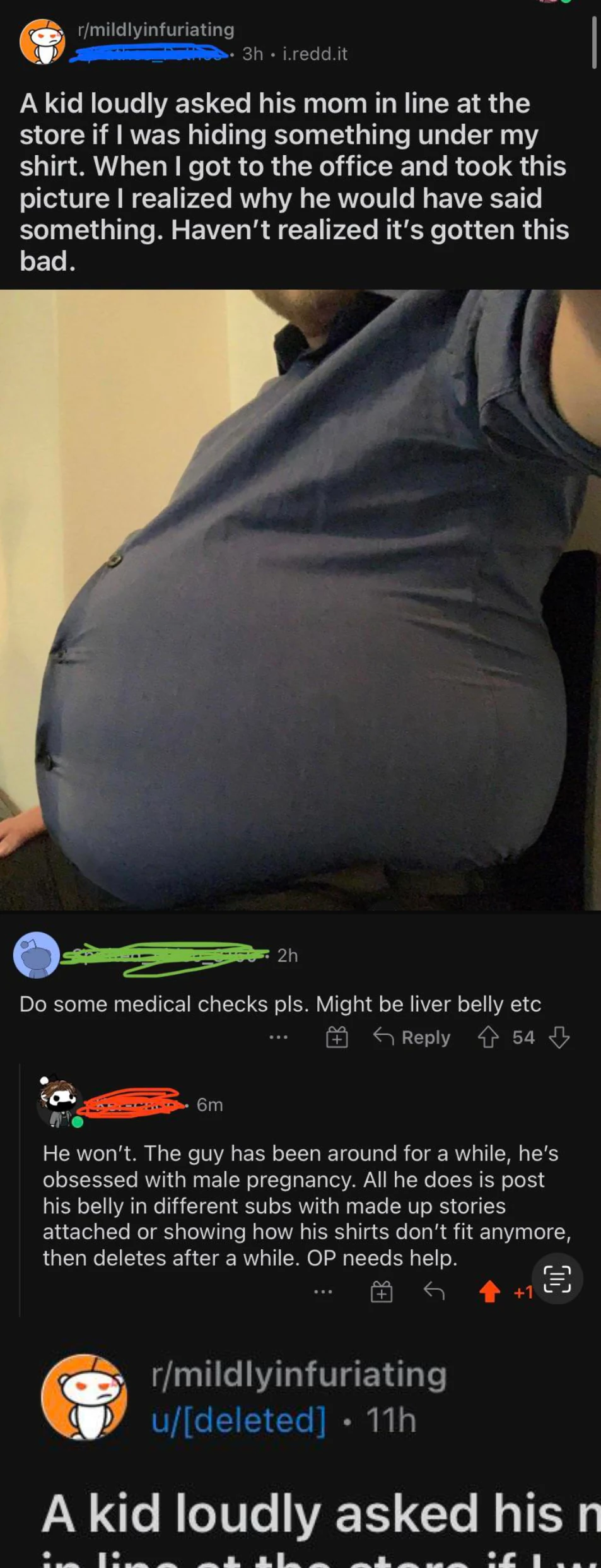

 posts photo of his oversized stomach with a bs backstory, redditor figures out he's a fetishist who gets off to posting his disgusting body on reddit
posts photo of his oversized stomach with a bs backstory, redditor figures out he's a fetishist who gets off to posting his disgusting body on reddit
- 9
- 62
https://camas.unddit.com/#{%22author%22:%22Pathos_Pothos%22,%22searchFor%22:1,%22resultSize%22:1000}
all his posts are photos of him being a disgusting blob with made-up stories





- 82
- 113
can guarantee the most clinically unhealthy person you know is a thin white woman who works out.
— Ally Maynard (@allymayn) October 11, 2022


- 17
- 24
this morning, The Pulse asks the important question: Can you eat $28 worth of fast food? https://t.co/tHrgoMA5Ko pic.twitter.com/0SBy0UDb6V
— Chris Branch (@cbranch89) October 13, 2022



- 12
- 30














- 2
- 9
https://old.reddit.com/r/stuffers
Not for long.
https://old.reddit.com/r/redditrequest/comments/y1jn1x/requesting_rstuffers/
Nobody is talking about this sadly.
Top Poster of the Day:

 GoldMemer
GoldMemer
Current Registered Users: 28,757
 BROWSE EFFORTPOSTS
SITE GUIDE
HOLES
PING GROUPS
BROWSE EFFORTPOSTS
SITE GUIDE
HOLES
PING GROUPS
/h/fatpeoplehate SETTINGS /h/fatpeoplehate LOG /h/fatpeoplehate MODS /h/fatpeoplehate EXILEES /h/fatpeoplehate FOLLOWERS /h/fatpeoplehate BLOCKERS